



200
评论
查看更多
密码过期或已经不安全,请修改密码
修改密码
壹生身份认证协议书
同意
拒绝
同意
拒绝
同意
不同意并跳过




2026年2月26-28日,2026年度美国临床肿瘤学会泌尿生殖系统肿瘤研讨会(2026 ASCO GU)正式召开,在这一泌尿肿瘤领域的年度盛会中,免疫检查点抑制剂相关研究再次成为焦点话题。如何看待免疫毒性与治疗效果之间的关系,几位学者分享了他们的观点。
Keypoints:
免疫检查点抑制剂(ICI)已改变泌尿生殖系统肿瘤的治疗格局,但也带来了独特的免疫介导毒性。
免疫毒性既常见又具有临床意义。近期研究表明,免疫相关不良事件与治疗结局改善呈正相关;然而,并非所有毒性都能同等预测获益。
早期发现和结构化处理irAE对于安全有效地使用ICI至关重要。

Dr. Nikita V. Baclig
UCLA
ICI已经改变了泌尿生殖系统恶性肿瘤的治疗格局。然而,它们的成功也伴随着代价。ICI毒性,也称为免疫毒性或irAE,与化疗毒性截然不同,因为它影响更广泛的器官系统,且在患者群体中不可预测地发生。因此,应对免疫毒性需要高度警惕,以便在副作用升级前发现并处理它们。矛盾的是,越来越多的证据表明,我们试图预防的各种毒性恰恰是疗效的标志。因此,临床医生在使用ICI时必须运用细致审慎的视角并仔细权衡,以平衡获益与伤害。

Dr. Leland F. Damron
UCLA
CheckMate-025 研究表明,与依维莫司相比,纳武利尤单抗治疗既往经治的转移性肾细胞癌患者可改善生存率,这是ICI 首次在肾细胞癌中显示出活性。此后不久,CheckMate-214 试验显示,纳武利尤单抗联合伊匹木单抗优于舒尼替尼,开启了当前标准治疗 ICI 双药方案作为转移性肾细胞癌一线治疗的时代。根据 KEYNOTE-564 试验,ICI 还被进一步应用于肾切除术后高危早期肾细胞癌的治疗,该试验显示,与安慰剂相比,帕博利珠单抗治疗改善了患者的总生存期。
ICI 也在膀胱癌治疗中占据关键地位。在非肌层浸润性膀胱癌中,帕博利珠单抗已被批准用于卡介苗难治性疾病,而 sasanlimab和度伐利尤单抗已被证明对新诊断的非肌层浸润性膀胱癌患者有效。
在肌层浸润性疾病的围手术期治疗中,度伐利尤单抗联合顺铂化疗是适合顺铂治疗患者的新标准治疗。对于拒绝或不适合顺铂治疗的患者,基于 EV-303 研究,维恩妥尤单抗联合帕博利珠单抗近期获得批准。在辅助治疗方面,根据 CheckMate-274 试验,对于因拒绝或对顺铂化疗反应不佳的高风险患者,纳武利尤单抗获批使用。同样,在辅助治疗中,帕博利珠单抗与安慰剂相比改善了无事件生存期,而阿替利珠单抗在循环肿瘤 DNA 检测阳性的患者中显示出膀胱切除术后的生存获益。在转移性背景下,新的前线标准治疗是帕博利珠单抗联合 nectin-4 抗体药物偶联物维恩妥尤单抗;然而,纳武利尤单抗联合顺铂化疗也可作为一线治疗。在此标准之前,基于JAVELIN Bladder-100研究,一线铂类化疗后通常使用阿维鲁单抗进行维持治疗。新型免疫联合疗法正在开发中,涉及的药物包括vepugratinib和维迪西妥单抗。
尽管 ICI 尚未被证明对前列腺癌、阴茎癌或睾丸癌有效,但帕博利珠单抗和纳武利尤单抗具有用于高度微卫星不稳定肿瘤的泛癌种适应证,因此罕见情况下可考虑作为难治性患者的治疗选择。

Dr. Dimitrios Stefanoudakis
UCLA

Ms. Marilena Iliopoulos
UCLA
ICI 的作用机制已被充分阐述,其核心是阻断癌细胞与 T 细胞之间的关键抑制信号。PD-1、PD-L1 和 CTLA-4 等免疫检查点蛋白通常与 T 细胞结合以阻断免疫系统对肿瘤的破坏。通过阻断这些检查点,ICI 可以恢复 T 细胞对抗癌细胞的活性。然而,这种免疫激活也可能错误地指向健康组织,产生类似于自身免疫的临床表现。免疫毒性部分由过度的细胞因子释放驱动,这会引发广泛的炎症、血管损伤和液体渗入组织,最终导致器官损伤。

Dr. Lidia P. Lopez
UCLA
免疫治疗与一系列发生频率不同的irAE相关。虽然最常受影响的器官部位包括皮肤、内分泌器官、肺和胃肠道,但任何器官都可能受累。泌尿生殖系统癌症患者中免疫毒性的发生率估计在35%到50%之间,其中约10%经历≥3级毒性。最常见的是皮疹、甲状腺功能减退和腹泻。最常见的严重毒性是腹泻、严重皮肤反应和丙氨酸氨基转移酶升高。其他较少见的毒性包括疲劳、其他内分泌功能障碍、风湿症状和肺炎。罕见的irAE,如神经系统综合征、眼毒性、心脏毒性和血管炎,见于1%至2%的患者。总体而言,有证据报告,免疫相关死亡率发生在0.26%的患者中,其中肺炎、肝功能衰竭和肝炎是最常见的死亡原因。

Dr. Alexandra Drakaki
UCLA
多项研究已证明 irAE 与免疫治疗的抗肿瘤效应之间存在正相关。在肾细胞癌中,一项回顾性系列研究显示,出现 irAE 的患者具有更优的总生存期和更长的至后续治疗时间。同样,在一个接受纳武利尤单抗治疗的389例患者队列中,irAE 的出现与生存获益之间存在强相关性。一项针对1747例尿路上皮癌患者的汇总分析也将irAE与改善的总生存期联系起来。然而,并非所有毒性都能同等预测获益:一项针对6148例肾细胞癌或尿路上皮癌患者的荟萃分析发现,经历irAE的患者总生存期和无进展生存期更好,但亚组分析显示,出现肺部 irAE或≥3级事件的患者总生存期更差。总的来说,尽管 irAE 可能与增强的治疗反应相关,但其异质性和严重毒性的风险凸显了对其机制深入理解和开发预测性临床工具的必要性。
早期识别和及时的免疫抑制干预对于获得最佳结局至关重要。大多数irAE为低级别,可以通过支持治疗进行管理。2 至3级事件通常需要皮质类固醇和治疗中断,而4级毒性则需要永久停药。尽管已有国家综合癌症网络和ASCO的管理指南,但由于许多社区机构难以接触到专科医生、治疗开始前基线实验室和诊断检测的不确定性,以及缺乏在治疗期间或治疗后监测动态irAE的标准化监测策略,及时识别仍然具有挑战性。
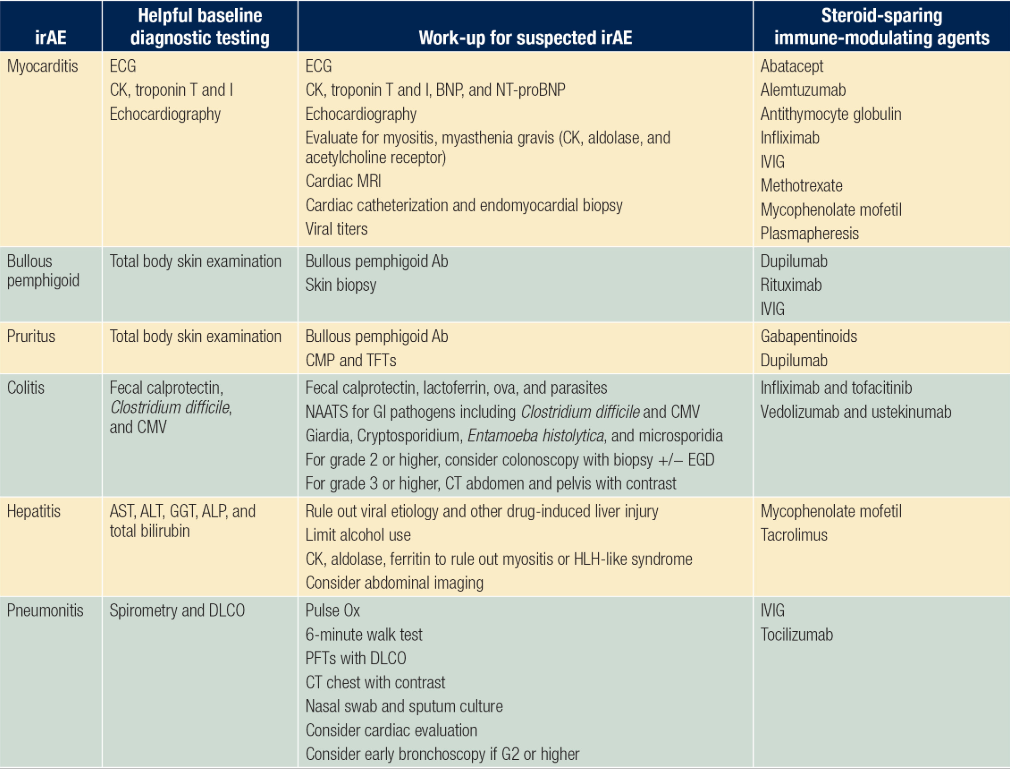
一个专家小组提出了首个用于早期检测的监测模式,包括基线实验室检查、肺功能检查、心电图、动态血氧饱和度监测以及详细的患者和家族自身免疫性疾病史。需要进一步的工作来验证和实施这种方法。皮质类固醇仍是治疗的基石,而对于类固醇难治性或危及生命的病例,根据器官特异性临床指南,越来越多地依赖于其他免疫调节剂。表格包含一个基于我们临床专业知识的早期检测和治疗模式。
缩略词: Ab, antibodies; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BNP, B-type natriuretic peptide; CK, creatine kinase; CMP, comprehensive metabolic panel; CMV, cytomegalovirus; DLCO, diffusing capacity for carbon monoxide; ECG, electrocardiogram; EGD, esophagogastroduodenoscopy; GGT, gamma-glutamyl transferase; GI, gastrointestinal; HLH, hemophagocytic lymphohistiocytosis; irAE, immune-related adverse event; IVIG, intravenous immunoglobulin; NAATS, nucleic acid amplification tests; NT-proBNP, N-terminal pro-BNP; PFT, pulmonary function test; TFT, thyroid function test.
ICI 重塑了泌尿生殖系统肿瘤学,同时也引入了一系列新的潜在严重毒性。免疫毒性既是代价,矛盾的是,也是治疗成功的标志。泌尿生殖系统癌症免疫治疗的未来不仅取决于完善治疗以最大化疗效,还取决于开发用于早期检测和管理 irAE 的系统。简而言之,只有当临床医生能够在不影响患者安全的情况下驾驭 ICI 的力量时,其全部潜力才能得以实现。
参考文献:
Motzer RJ, Escudier B, McDermott DF, et al; CheckMate 025 Investigators. Nivolumab versus everolimus in advanced renal-cell carcinoma. N Engl J Med. 2015;373(19):1803-1813.
Motzer RJ, Tannir NM, McDermott DF, et al; CheckMate 214 Investigators. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med. 2018;378(14):1277-1290.
Choueiri TK, Tomczak P, Park SH, et al; KEYNOTE-564 Investigators. Overall survival with adjuvant pembrolizumab in renal-cell carcinoma. N Engl J Med. 2024;390(15):1359-1371.
Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): an open-label, single-arm, multicentre, phase 2 study. Lancet Oncol. 2021;22(7):919-930.
Shore ND, Powles TB, Bedke J, et al. Sasanlimab plus BCG in BCG-naive, high-risk non-muscle invasive bladder cancer: the randomized phase 3 CREST trial. Nat Med. 2025;31(8):2806-2814.
De Santis M, Palou Redorta J, Nishiyama H, et al; POTOMAC Investigators. Durvalumab in combination with BCG for BCG-naive, high-risk, non-muscle-invasive bladder cancer (POTOMAC): final analysis of a randomised, open-label, phase 3 trial. Lancet. 2025;406(10516):2221-2234.
Powles T, Catto JWF, Galsky MD, et al; NIAGARA Investigators. Perioperative durvalumab with neoadjuvant chemotherapy in operable bladder cancer. N Engl J Med. 2024;391(19):1773-1786.
Galsky MD, Hoimes CJ, Necch A, et al. Perioperative pembrolizumab therapy in muscle-invasive bladder cancer: phase III KEYNOTE-866 and KEYNOTE-905/EV-303. Future Oncol. 2021;17(24):3137-3150.
U.S. Food and Drug Administration. FDA approves pembrolizumab with enfortumab vedotin-ejfv for muscle invasive bladder cancer. FDA.gov. November 21, 2025. Accessed December 17, 2025. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-pembrolizumab-enfortumab-vedotin-ejfv-muscle-invasive-bladder-cancer.
Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021;384(22):2102-2114.
Apolo AB, Ballman KV, Sonpavde G, et al. Adjuvant pembrolizumab versus observation in muscle-invasive urothelial carcinoma. N Engl J Med. 2025;392(1):45-55.
Powles T, Kann AG, Castellano D, et al; IMvigor011 Investigators. ctDNA-guided adjuvant atezolizumab in muscle-invasive bladder cancer. N Engl J Med. Published online October 20, 2025.
Powles T, Valderrama BP, Gupta S, et al; EV-302 Trial Investigators. Enfortumab vedotin and pembrolizumab in untreated advanced urothelial cancer. N Engl J Med. 2024;390(10):875-888.
Powles T, Park SH, Voog E, et al. Avelumab maintenance therapy for advanced or metastatic urothelial carcinoma. N Engl J Med. 2020;383(13):1218-1230.
O’Malley DM, Bariani GM, Cassier PA, et al. Pembrolizumab in patients with microsatellite instability-high advanced endometrial cancer: results from the KEYNOTE-158 study. J Clin Oncol. 2022;40(7):752-761.
Boussiotis VA. Molecular and biochemical aspects of the PD-1 checkpoint pathway. N Engl J Med. 2016;375(18):1767-1778.
Bou Zerdan M, Moussa S, Atoui A, Assi HI. Mechanisms of immunotoxicity: stressors and evaluators. Int J Mol Sci. 2021;22(15):8242.
Mercinelli C, Carli C, Di Vita R, Oliveri M, Galli L, Necchi A. Immunotherapy toxicities in genito-urinary cancers: insights and challenges for clinicians. Curr Opin Urol. 2025;35(4):461-466.
Wu Z, Chen Q, Qu L, et al. Adverse events of immune checkpoint inhibitors therapy for urologic cancer patients in clinical trials: a collaborative systematic review and meta-analysis. Eur Urol. 2022;81(4):414-425.
Mar N, Slaught M, Kaakour D, Azizi A, Valerin JB. Distribution of immune-related adverse events (irAEs) across genitourinary (GU) malignancies. J Clin Oncol. 2022;40:6s (suppl; abstr 470).
Thapa B, Roopkumar J, Kim AS, et al. Incidence and clinical pattern of immune related adverse effects (irAE) due to immune checkpoint inhibitors (ICI). J Clin Oncol. 2019;37:15s (suppl; abstr e14151).
Maher VE, Fernandes LL, Weinstock C, et al. Analysis of the association between adverse events and outcome in patients receiving a programmed death protein 1 or programmed death ligand 1 antibody. J Clin Oncol. 2019;37(30):2730-2737.
Eggermont AMM, Kicinski M, Blank CU, et al. Association between immune-related adverse events and recurrence-free survival among patients with stage III melanoma randomized to receive pembrolizumab or placebo: a secondary analysis of a randomized clinical trial. JAMA Oncol. 2020;6(4):519-527.
Cortellini A, Buti S, Agostinelli V, Bersanelli M. A systematic review on the emerging association between the occurrence of immune-related adverse events and clinical outcomes with checkpoint inhibitors in advanced cancer patients. Semin Oncol. 2019;46(4-5):362-371.
Elias R, Levonyak N, Christie A, et al. A real-world experience of immune checkpoint inhibitors (ICI) in metastatic renal cell carcinoma (mRCC). J Clin Oncol. 2020;38:6s (suppl; abstr 647).
Verzoni E, Cartenì G, Cortesi E, et al; Italian Nivolumab Renal Cell Cancer Early Access Program group. Real-world efficacy and safety of nivolumab in previously-treated metastatic renal cell carcinoma, and association between immune-related adverse events and survival: the Italian expanded access program. J Immunother Cancer. 2019;7(1):99.
Zhang Y, Chen J, Liu H, et al. The incidence of immune-related adverse events (irAEs) and their association with clinical outcomes in advanced renal cell carcinoma and urothelial carcinoma patients treated with immune checkpoint inhibitors: a systematic review and meta-analysis. Cancer Treat Rev. 2024;129:102787.
Puzanov I, Diab A, Abdallah K, et al; Society for Immunotherapy of Cancer Toxicity Management Working Group. Managing toxicities associated with immune checkpoint inhibitors: consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J Immunother Cancer. 2017;5(1):95.
Özdemir BC, Espinosa da Silva C, Arangalage D, et al. Multidisciplinary recommendations for essential baseline functional and laboratory tests to facilitate early diagnosis and management of immune-related adverse events among cancer patients. Cancer Immunol Immunother. 2023;72(7):1991-2001.
Schneider BJ, Naidoo J, Santomasso BD, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update. J Clin Oncol. 2021;39(36):4073-4126.
本文整理自:ASCO Daily News.
查看更多
 中国医学论坛报
中国医学论坛报 壹生
壹生 今日肿瘤
今日肿瘤 今日循环
今日循环 今日糖尿病
今日糖尿病 今日口腔
今日口腔 全科周刊
全科周刊 脱贫地区农副产品网络销售平台
脱贫地区农副产品网络销售平台
京公网安备 11010202008182号
| 互联网新闻信息服务许可证编号:10120190017